Executive summary
In 2026 in the United States, daylight saving time runs from March 8 at 2:00 a.m. (local time) to November 1 at 2:00 a.m. (local time). National Institute of Standards and Technology publishes these official DST rules and dates.
The “spring forward” shift is not just a clock change. It is a one-hour mismatch between your body clock and the schedule you’re suddenly expected to follow. That mismatch shows up as real sleep loss in real-world measurements: a large UK accelerometer study found about 60–65 minutes less sleep on the DST Sunday compared with nearby Sundays.
The first week after spring forward is also when public-health ripple effects show up most often in the news and in research: more fatigue, more errors, and measurable increases in some risks like fatal car crashes and a small bump in heart attack risk in pooled analyses.
The simplest, best-supported strategy is boring but effective: start shifting in advance (even a few days), use morning light to “pull” your body clock earlier, and reduce bright evening light so your brain can wind down on time. Centers for Disease Control and Prevention summarizes this “15–20 minutes earlier” approach in its DST adaptation guidance.
Why spring forward disrupts sleep in plain English

Daylight saving time affects sleep because your sleep system runs on light and routine, not on what your phone says.
Your circadian rhythm (your internal clock). Your body has an internal timing system that roughly tracks a 24-hour day. Light and dark are the strongest signals that set this clock, but meal times, activity, and social schedules also matter. National Institutes of Health explains that light/dark has the biggest influence on circadian rhythms and that other factors (like food intake and activity) can shift them, too.
When the clocks jump forward, sunrise is suddenly “later” by the clock. Many people end up getting less morning light (which normally helps wake you up) and more light in the evening (which pushes your sleep later). Mainstream explainers describe this as a body-clock conflict that feels like a mini jet lag, especially in spring.
Melatonin (your “darkness hormone”). Melatonin is a hormone your brain makes in response to darkness. Exposure to light at night can block melatonin production, which makes it harder to feel sleepy at the right time. NIH explicitly states both points: darkness triggers melatonin, and light at night can block it.
DST can worsen a common pattern: later sunsets encourage later screen time and later bedtimes, while the next morning still demands an earlier wake time. The result is sleep debt.
Sleep stages (why the “lost hour” can feel extra rough). You don’t sleep in one uniform block. You cycle through REM and non-REM sleep in repeating loops about every 80–100 minutes.
In plain terms: the last part of the night often contains more REM, and many people feel the “spring forward” hit as groggier mornings and shakier focus because the end of sleep gets squeezed.
Key peer-reviewed findings with one-line effect sizes
- Sleep loss on the spring DST Sunday is real and often close to an hour. In a large accelerometer dataset (UK Biobank), average sleep duration was ~65 minutes shorter on the spring DST Sunday versus the Sunday before, and ~61 minutes shorter versus the Sunday after. (de Lange et al., 2025)
- Teens lose meaningful sleep for days, not just one night. In a high-school actigraphy natural experiment, students slept ~32 minutes less per school night in the week after spring forward (about 2 hours 42 minutes total for the school week). (Medina et al., 2015)
- Fatal crash risk rises after spring forward in major U.S. data. A chronobiology analysis of U.S. fatal traffic accidents found the spring transition was associated with a ~6% increase in fatal traffic accident risk. (Fritz et al., 2020)
- Heart attack risk shows a small pooled increase after spring forward. A systematic review/meta-analysis reported a pooled relative risk of acute myocardial infarction of ~1.04 (≈4% higher) after DST onset (spring). (Hurst et al., 2024)
- Not everyone adapts at the same speed. In an NIH-covered wearable-tracker study of medical residents, “early risers” adjusted in a few days, while “late” chronotypes showed disruption about a week later. (NHLBI/NIH summary, 2021)
Simple comparison table of designs and outcomes
| Source (type) | Who/where | What was measured | Plain-language outcome |
|---|---|---|---|
| de Lange et al., 2025 (accelerometers) | Adults in UK Biobank | Objective sleep duration around DST | Spring DST Sunday: ~60–65 minutes less sleep |
| Medina et al., 2015 (actigraphy + performance tests) | High school students | Weeknight sleep + vigilance | ~32 minutes less sleep/night for the following school week + worse vigilance |
| Fritz et al., 2020 (registry analysis) | U.S. fatal crash data | Fatal traffic accidents | Spring forward week: ~6% higher fatal crash risk |
| Hurst et al., 2024 (meta-analysis) | Studies from multiple countries | Acute myocardial infarction | Spring onset: pooled ~4% higher AMI risk |
| NHLBI/NIH 2021 (wearables + genetics summary) | Medical residents | Sleep schedule disruption and timing | Early chronotypes: days; late chronotypes: about a week for noticeable disruption |
What official sources and major coverage emphasize
This is the “practical authority layer”: what public agencies and widely read outlets consistently highlight.
CDC (sleep + DST prep). CDC’s DST guidance stresses that the light/time shift can disrupt circadian rhythms and sleep and recommends preparing by shifting bedtime earlier by 15–20 minutes per night and shifting other “time cues” (like dinner and exercise timing) earlier as well.
Separately, CDC’s sleep guidance includes concrete sleep-hygiene steps that matter during DST week: keep a regular schedule, get natural light earlier in the day, avoid artificial light near bedtime, and avoid caffeine later in the day.
NIH (simple physiology). NIH’s public-facing materials support the core mechanism that most news explainers rely on: circadian rhythms are strongly shaped by light/dark, and melatonin is the darkness-triggered signal that evening light can block.
WHO (sleep as a health behavior). The World Health Organization does not publish DST-specific sleep instructions, but it does publish formal sleep guidance as part of 24‑hour health behavior recommendations in early childhood (sleep + activity + sedentary time). That matters because DST disrupts the same thing these guidelines try to protect: consistent daily rhythms.
Sleep societies (policy stance + common-sense steps). American Academy of Sleep Medicine has repeatedly argued that eliminating seasonal clock changes—favoring permanent standard time—better matches human circadian biology, and it also publishes practical steps (gradual schedule shift, morning light, consistent sleep).
National Sleep Foundation similarly connects the clock change with sleep disruption and safety concerns (including roadway risk) and promotes incremental schedule shifts, morning daylight exposure, and short naps when needed.
Medical organizations and major reporting echo the same theme. American Medical Association has publicly supported ending DST and frames spring forward as a public-health and safety issue linked with cardiovascular morbidity and missed care patterns.
American Heart Association messaging emphasizes that sleep loss and circadian disruption can strain heart/brain health and ties inadequate sleep to broader risks (including depression and cognitive issues).
Major outlets such as Associated Press and TIME repeatedly describe spring forward as harder than fall back because it combines darker mornings with brighter evenings, making it easier to drift later while still needing to wake earlier.
Public-health impacts in simple terms
Spring forward matters because “a little less sleep” is not evenly distributed across people or days. The impact clusters in the first days and hits safety-critical activities.
Accidents and errors. The cleanest, most widely cited safety outcome is crash risk: a large analysis found ~6% higher fatal crash risk after the spring transition.
This is why many official and mainstream sources treat the first Monday–Wednesday after spring forward as a higher-risk window for drowsy driving and impaired focus.
Heart attacks and stroke. The average person’s absolute risk stays low, but at the population level, small relative shifts can still matter. Meta-analyses suggest a small (~4%) increase in heart-attack risk after spring DST onset.
The American Heart Association and other public health explainers frame the mechanism in plain language: sleep loss and body-clock disruption can alter stress hormones, blood pressure patterns, and inflammation signals—especially relevant for people already at cardiovascular risk.
Mood and mental bandwidth. News explainers and public-health sources consistently note irritability, low mood, and worse focus after spring forward, which fits what sleep science already knows about short sleep and poor sleep quality.
The main point for readers is practical: DST can tilt you into a short-term “thin margin” state—less patience, worse decision-making, and more mistakes.
Productivity and work performance. There is mainstream coverage that the time change can cost real output: reports highlight short-term drops in focus and productivity after spring forward.
A university summary of newer research argues the effect may last longer than a single day for some workers, particularly for early-morning performance. University of Oregon
My DST sleep checklist for real life
I treat spring forward like a predictable one-hour eastbound trip that I didn’t choose. The goal is not perfection. The goal is reducing the mismatch and protecting the first few days.
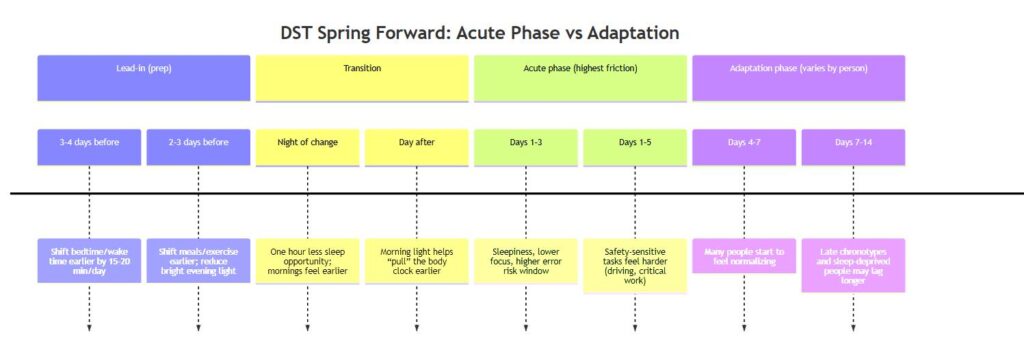
Before the shift
- Shift bedtime and wake time earlier by 15–20 minutes per day for at least 3–4 days.
- Shift “time cues” earlier too: dinner, workouts, and even the start of your wind-down routine.
- Bank sleep. Go into the weekend well-rested. CDC notes that many adults already get less than recommended sleep, which makes DST harder.
- Start dimming evenings: reduce bright indoor lighting and screens close to bedtime so melatonin isn’t being blocked.
The day of the change
- Set clocks forward the night before so the morning isn’t chaotic.
- Get outside light in the morning even if it’s cloudy; multiple official and mainstream sources stress morning light as the fastest “reset” cue.
- Keep bedtime close to your target. Avoid “revenge scrolling” into the brighter evening.
The first week after
- Protect mornings as a higher-risk zone for drowsy driving and mistakes. The safety signal in crashes is strongest right after spring forward.
- Use a short nap only if needed: 20–30 minutes, earlier in the day.
- Put a hard cutoff on caffeine. CDC recommends avoiding caffeine in the afternoon/evening, and controlled research shows caffeine can disrupt sleep even when taken 6 hours before bed.
- Keep wake time steady. A consistent wake time is the anchor that helps your circadian timing settle.
- Use light intentionally: bright mornings, calmer/dimmer evenings. That direction is consistent across CDC guidance and major explainers.
FAQ
Does daylight saving time really cause sleep loss?
Yes. Objective monitoring shows a meaningful drop in sleep on the spring DST night—often on the order of ~30–65 minutes on average, depending on the dataset. (de Lange et al., 2025)
Why is spring forward harder than fall back?
Spring forward combines two problems: you lose an hour of sleep opportunity immediately, and the brighter evenings/darker mornings shift light exposure in a direction that can make it easier to drift later while still needing to wake earlier. (AP, 2025; TIME, 2025–2026)
How long does it take to adjust to DST?
Many people feel better within several days, but not everyone adapts at the same speed. NIH-reported wearable research suggests earlier chronotypes adjust in a few days, while later chronotypes can feel disruption a week later. (NHLBI/NIH, 2021)
Does DST increase the risk of heart attacks?
Pooled research finds a small average increase after spring forward—about ~4% higher relative risk in a meta-analysis. (Hurst et al., 2024)
Does DST increase car crashes?
A large U.S. analysis of fatal traffic accidents found an association of about ~6% higher fatal crash risk after the spring transition. (Fritz et al., 2020)
Which places don’t observe DST in the U.S.?
The best-known exceptions are Hawaii and most of Arizona (plus several U.S. territories), which stay on standard time year-round. (AP, 2025; TIME, 2026)